Click here to download a pdf version of this Memorandum
Steven A. Camarota is the Director of Research at the Center for Immigration Studies.
Based on our analysis of Census Bureau data, we estimate that there are 6.6 million uninsured illegal immigrants in the United States who could be covered by the new health care reform bill (HR 3200). Even though HR 3200 states that illegal immigrants are not eligible for the proposed taxpayer-funded affordable premium credits, there is nothing in the bill to enforce this. An amendment was defeated in committee that would have required the use of the Systematic Alien Verification for Entitlements (SAVE) program, used by almost all other means-tested programs of this kind.
Among the findings:
- We estimate that there were 6.6 million illegal immigrants without health insurance in 2007 who had incomes below 400 percent of the poverty level, which is the income ceiling for the proposed affordable premium credits.
- If all uninsured illegal immigrants with incomes below 400 percent of poverty received the proposed credits, the estimated cost to the federal government would be $30.5 billion annually.
- We estimate the current cost of treating uninsured illegal immigrants at all levels of government to be $4.3 billion a year, primarily at emergency rooms and free clinics.
- On July 16, an amendment by Rep. Dean Heller (R-Nev.) that would have required use of the SAVE program to prevent illegal immigrants from receiving the affordable premium credits was defeated by the House Ways and Means Committee.
- At present, 71 other means-tested federal programs require use of the SAVE system to prevent illegal immigrants and other ineligible non-citizens from accessing them.
- Even though there is no mechanism to prevent enrollment, it is likely that many income-eligible illegal immigrants would not enroll out of fear or lack of knowledge of the new programs. Thus, the actual costs could be less than the $30.5 billion estimated above. However, if illegal immigrants are legalized, a much larger percentage can be expected to enroll, with a corresponding increase in costs.
- Uninsured illegal immigrants tend to use less health care on average than others without health insurance because they tend to be young. This fact is incorporated into our current cost estimate of $4.3 billion. However, government-provided affordable premium credits paid to insurance companies would be the same for everyone, regardless of age or preexisting conditions. Therefore, the younger age of illegals does not result in lower average costs for taxpayers for this program.
- It is also worth noting that we estimate that 38 percent of illegal immigrants had health insurance in 2007 and that there are at least 360,000 uninsured illegal immigrants with incomes above 400 percent of poverty who would not qualify for benefits under HR 3200.
- Illegal immigrants could benefit from the expansion of Medicaid under HR 3200. The bill does not require identity verification for those claiming U.S. birth. Of illegal immigrants with incomes under 400 percent of poverty, about half earn less than 133 percent of poverty, which is the new ceiling for Medicaid eligibility.
Lack of Enforcement in HR 3200
The America’s Affordable Health Choices Act of 2009 (HR 3200) is extremely complex and there’s no way to know how the bill ultimately will be implemented. First, it is unclear if illegal immigrants will be required to have health insurance, as would citizens and legal immigrants (green card holders). In its summary of the bill, the Congressional Research Service (CRS) states, “Under HR 3200, all legal permanent residents (LPRs), non-immigrants, and unauthorized aliens who meet the substantial presence test… would be required to obtain health insurance.”1 Substantial presence is defined as having been in the United States for at least 31 days during the current year and at least 183 days during the current year and previous two years. No mention is made of legal status in the legislation for determining substantial presence.
The legislation offers affordable premium credits, or more simply affordability credits, to persons with low incomes who meet the substantial presence criteria. Under HR 3200, individuals would use the newly created Health Insurance Exchange to get affordability credits or to enroll in the to-be-created government-provided health insurance program often referred to as the “public option.” The credits are based on a sliding scale, with lower-income people getting a larger credit. The income ceiling for the credits and public option is 400 percent of the poverty level. Section 246 of HR 3200 states, “Nothing in this subtitle shall allow federal payments for affordability credits on behalf of individuals who are not lawfully present in the United States.”2 But as CRS points out, “HR 3200 does not contain any restrictions on non-citizens — whether legally or illegally present, or in the United States temporarily or permanently — participating in the Exchange.”3 So it would seem that illegal immigrants, along with some temporary workers and visitors, would be required to have insurance and could use the Exchange, despite a bar on them receiving taxpayer-financed affordable premium credits.
Even so, the bill does not include any means of determining legal status for those attempting to receive the affordability credits or the public option. Most similar means-tested programs require use of the Systematic Alien Verification for Entitlements (SAVE) program to prevent illegal immigrants or other ineligible non-citizens from getting benefits. The SAVE program is currently used to verify immigrant eligibility for 71 other means-tested programs of this kind. However, on July 16, an amendment by Rep. Dean Heller (R-Nev.) that would have required the use of the SAVE program to prevent illegal immigrants from receiving the affordability credits was defeated by the House Ways and Means Committee. At present, there seems little to prevent illegal immigrants from accessing the proposed taxpayer-subsidized health insurance.
Estimating the Illegal Population
To estimate the number of illegal immigrants in the United States, we used the March 2008 Current Population Survey (CPS), collected by the Census Bureau. The March survey, also called the Annual Social and Economic Supplement, is one of the best sources of information on the foreign-born, who also can be referred to as immigrants.4 The CPS does not include persons in “group quarters,” such as prisons and nursing homes. The March 2008 CPS shows 37.3 million immigrants in the country. It is well established that illegal aliens do respond to government surveys such as the Current Population Survey. While the CPS does not ask the foreign-born if they are legal residents of the United States, the Urban Institute, the Department of Homeland Security (DHS), former INS, Pew Hispanic Center, and the Census Bureau all have used socio-demographic characteristics in the data to estimate the size of the illegal alien population. We follow this same approach. Our best estimate is that the March 2008 CPS indicates a population of 10.5 million to 10.9 million illegal aliens, with 10.7 million as the middle value.5 It must be remembered that this estimate only includes illegal aliens captured by the March CPS, not those missed by the survey. By design, this estimate is consistent with those prepared by the Department of Homeland Security and others.6 The Department of Homeland Security assumes an undercount of 10 percent in Census Bureau data.7
Uninsured Illegal Immigrants
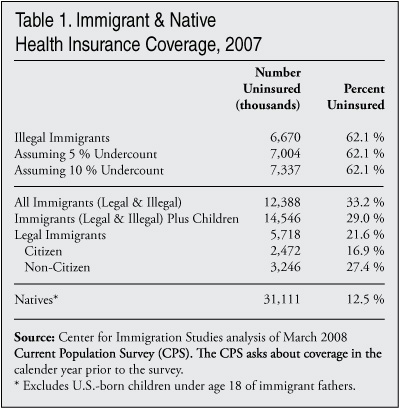
Table 1 reports our estimates of the uninsured illegal immigrant population with no adjustment for undercount, with a 5 percent upward adjustment for undercount, and with a 10 percent upward adjustment for undercount. The CPS asks respondents about health insurance coverage in the calendar year immediately prior to the survey. Thus the 2008 data provide information about health coverage in 2007. Based on the 2008 March CPS, we estimate that 6.67 million out of the 10.7 million illegal immigrants found by the survey were uninsured in 2007. In an earlier study based on 2007 data, we estimated that 7.25 million illegal immigrants were uninsured in 2006.8 Part of the reason for the decline is that the overall number of illegal immigrants in the country declined between 2007 and 2008. In addition, we estimate that there was a small decline in the share of illegal immigrants who were uninsured, from 64 percent in 2006 (2007 data) to 62 percent in 2007 (2008 data). It is worth noting that we estimate that 38 percent of illegal immigrants had insurance in 2007, typically through an employer or through a spouse who had employment-based health insurance.
Cost of Covering Illegal Immigrants
Our cost estimate focuses on the affordability credits. To help people purchase insurance, HR 3200 would provide a credit, or perhaps more accurately a voucher, to buy health insurance to those with incomes between 133 percent and 400 percent of the official poverty level. The size of the voucher would be determined by a sliding scale based on income.9 People could use the credits to buy insurance from a private company or, if they chose, could enroll in a new government-run health insurance system that the bill would create. This new government-run insurance is often referred to as the public option in the media. Under HR 3200, those with incomes below 133 percent of poverty are supposed to be enrolled in Medicaid, which the bill would expand. Medicaid provides health insurance free of charge. In our estimates we assume that those illegal immigrants with incomes below 133 percent of poverty would not enroll in Medicaid because they are barred from this program by existing law. As will be discussed later, however, HR 3200 would weaken the identity requirements for enrolling in Medicaid and may make it easier for illegal immigrants to enroll in the program fraudulently.
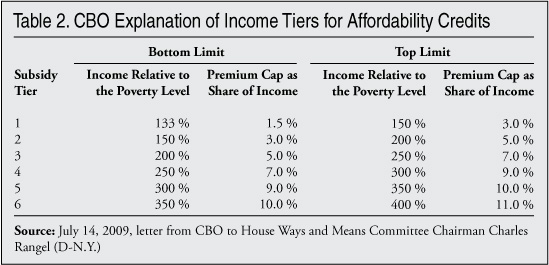
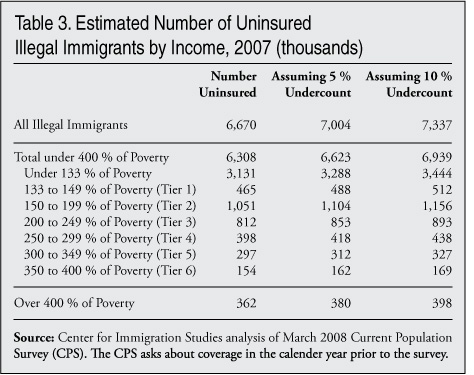
The Congressional Budget Office (CBO) has estimated that the average cost to the federal government for affordability credits for each subsidized enrollee will be $4,600 in 2014, when the program would begin, and that this will grow to $6,000 per enrollee by 2019.10 The bill envisions a sliding scale for the credits based on income. Table 2 shows the CBO’s theory of how income tiers might work based on their reading of the bill.11 While it is not entirely clear how the sliding scale would work in practice, Table 2 provides a good estimate. The table shows that for those with incomes between 133 percent and 150 percent of poverty, the affordability credits would limit premiums to between 1.5 percent and 3 percent of a recipient’s income. The federal government would make up the rest of the insurance costs. For those with incomes of 350 to 400 percent of poverty, Table 2 shows that the health insurance premiums would not exceed 10 to 11 percent. Table 3 shows our estimates, based on the CPS, for the number of illegal immigrants without health insurance in each income tier. The CPS shows that there are a total of 6.3 million uninsured illegal immigrants with incomes below 400 percent of poverty. If we assume a 5 percent undercount in the CPS, to be conservative, then there are 6.6 million income-eligible illegal immigrants without health insurance in the country. As Table 3 shows, about half of uninsured lower-income illegal immigrants have incomes less than 133 percent of poverty and half earn between 133 percent and 400 percent of poverty. Since illegal immigrants tend to be on the low side of the income distribution they can be expected to receive a credit that is somewhat higher than the $4,600 average estimated by CBO. In this analysis however, we assume that illegal immigrant enrollees would receive the average credit.
If all uninsured illegal immigrants with incomes under 400 percent of poverty received affordability credits, the cost to the federal government would be between $29 billion and $31.9 billion. This figure reflects the average credit as estimated by CBO multiplied by the number of uninsured illegal immigrants. The $29 billion figure assumes no undercount of the illegal population in the CPS and the $31.9 billion estimate assumes a 10 percent undercount. The middle-range value is $30.5 billion, which assumes a 5 percent undercount.
This estimate may seem high relative to the total cost estimates for HR 3200 from CBO and others.12 But it must be remembered that although the costs of covering the low-income uninsured are very high, the bill contains several provisions that shift money away from Medicare and increase taxes on some businesses and it assumes costs savings that are supposed to offset some of the very high costs of providing health care subsidies to low-income U.S. residents. But cost shifting and savings do not change the fact that if more uninsured people sign up for the affordability credits, costs must increase accordingly. Our $30.5 billion estimate assumes that all income-eligible illegal immigrants will sign up for the affordability credits. However, many illegals would be expected not to enroll in the new program out of fear or lack of knowledge, even if there is no enforcement mechanism. Thus, the actual costs could be less than the $30.5 billion estimated above. Of course, this would change if illegal immigrants were legalized
In general uninsured illegal immigrants are younger than the average uninsured native-born person or legal immigrant.13 Therefore, they should use significantly less in health care. But the affordability credits paid to insurance companies are explicitly designed not to adjust for age or preexisting conditions so the cost of the credit would be the same for uninsured illegal immigrants as for anyone else. What insurance companies ultimately pay to health care providers for illegal immigrants may end up being less on average than what it pays out for others. But the size of the credit from the government and the resulting cost to taxpayers is the same for illegal immigrants, legal immigrants, and natives, regardless of age or health status.
A central feature of HR 3200 is that insurance companies have to charge the same for every person, regardless of age or other health risk factors, and the subsidy from the government is also the same for every person. However, if illegal immigrants enroll in the new government-provided insurance program, then the younger age of illegal immigrants should result in lower costs for taxpayers than if they were enrolled in a private insurance plan. If illegal immigrants enroll in the public option, the government is bearing the costs directly and the younger age and generally good health of illegal immigrants should result in lower costs than would be the case if they were using affordability credits to buy private insurance. Even so, the costs of directly providing health care to millions of illegal immigrants through the public option would still run into the billions of dollars.14 At present, it is unclear if the pubic option will even be included in the final bill, and it is also unclear what share of illegals might be expected to enroll in the program.
Medicaid Expansion
Earlier this year, when Congress made Medicaid available to more children, it also made it easier to falsely claim U.S. birth. A person who claims to have been born in the United States now simply has to provide a Social Security number and name to enroll in Medicaid. In the past, documents like birth certificates and driver’s licenses would have been required for those claiming U.S. birth. Use of these documents ensures that the person enrolling is actually the person whose name and Social Security number are being submitted. Efforts to require the use of identity documents for those asserting U.S. birth were defeated at that time.
The same thing happened with the expansion of Medicaid under HR 3200. On July 30, an amendment by Rep. Nathan Deal (R-Ga.) stating that the use of identity documents was still required for those claiming U.S. birth was defeated by the House Energy and Commerce Committee. It is important to note that Medicaid enrollment is still supposed to require use of the SAVE program for people claiming to be qualified aliens. A qualified alien is a green card holder who has been in the country long enough to enroll in Medicaid or is a refugee or some other non-citizen allowed to enroll in the program. Naturalized U.S. citizens go through a different process to verify eligibility. But the lack of identity verification creates ambiguity and it is possible this could allow illegal immigrants, who commonly use stolen identities, to enroll in Medicaid.
Costs of Legalization
People without health insurance do receive health care, though it is not always adequate or timely. Nor do they typically receive as much care as they would if they had insurance. Charities and health care providers absorb some of the costs of treating the uninsured and the uninsured themselves pay for a significant part of their own care. But the Kaiser Family Foundation estimates that federal, state, and local governments spend $42.9 billion a year for treatment of the uninsured.15 As already indicated, based on the 2008 CPS we estimate that the number of illegal immigrants without health insurance is 6.67 million, or 14.6 percent of all the uninsured people in the country.16 If we adjust this estimate upward by 10 percent to account for those missed by the CPS, then uninsured illegal immigrants account for 15.6 percent of all uninsured U.S. residents.17
Although illegal immigrants are about 15 percent of the uninsured, they do not account for 15 percent of the costs of treating the uninsured. Illegal immigrants tend to be younger on average than others without health insurance, which reduces their health care use. Also they are unable to use several relatively large programs that are included in the $42.9 billion figure for providing care to the uninsured, such as programs for uninsured American Indians and veterans. The only factor that tends to elevate costs for uninsured illegal immigrants is that they have much higher fertility rates compared to all other segments of the uninsured population and even routine births in hospitals are very costly. Although illegal immigrants are estimated to be 4 percent of the total U.S. population, they account for almost 10 percent of all births in the United States.18 Nevertheless, we estimate that despite their 15 percent share of the uninsured, illegal immigrants account for only 10 percent of all governmental costs of treating the uninsured, or $4.3 billion annually.19 While this is a substantial dollar figure, it is much less than if they had government-provided insurance, particularly if they receive the new affordability credits. Although taxpayer-financed health insurance to illegal immigrants would be much more costly than the status quo, it is almost certainly the case that if illegal immigrants were given health insurance it would improve their health care outcomes. This is, of course, true for any uninsured segment of the U.S. population.
President Obama and others have indicated their strong desire to legalize those in the country illegally with the hope that this would help solve the problem of uninsured illegal immigrants. It is certainly correct that legalizing illegal immigrants and allowing them to receive the new affordability credits, public option plan, or perhaps enrolling in Medicaid would dramatically increase the share with insurance. However, it would also dramatically increase costs to taxpayers, which should be part of any legalization discussion.
It is important to note that the average wages for illegal immigrants should rise if they are legalized, and this should reduce the fraction who have incomes under 400 percent of poverty and could receive taxpayer-financed health care. How much their wages would go up is a matter of some debate. Illegal immigrants tend to be poor, but this is mainly due to the large share with relatively little education and limited English skills. The best research shows that wages for those legalized by the 1986 amnesty rose 6 percent within a few years as a result of the legalization.20 However, other research indicates that the increase in wages from the 1986 amnesty may have been larger.21 Given the very low incomes of most illegal immigrants, the rise in wages would have to be very substantial to move a significant number above the income thresholds for receiving insurance subsidies in HR 3200. For a family of four, 400 percent of poverty is about $88,000 a year. On the other hand, moving someone from a lower income tier to a higher income tier would save taxpayers money. As Table 3 shows, 54 percent of uninsured illegal immigrants have incomes below 150 percent of poverty compared to 40 percent of all other persons without health insurance. Uninsured illegal immigrants are more concentrated at the bottom end of the income distribution.
Another way to think about the impact of legalization is to examine the situation of non-citizen legal immigrants (green card holders) who are less educated. We estimate that 81 percent of all adult illegal immigrants have no more than a high school education based on the 2008 CPS.22 If illegal immigrants were legalized, they would in effect become less-educated green card holders (legal immigrants). Based on the 2008 data, we find that 35 percent of adult green card holders with no more than a high school degree were uninsured. While this is still very high, about three times the rate for native-born Americans, it is much better than the 62 percent uninsurance rate we find for illegal immigrants. However, the primary difference is that 27 percent of less-educated green card holders are on Medicaid, while virtually no illegal immigrants use that program. This means that the share of less-educated legal immigrants who are uninsured or on Medicaid is almost the same as the share of illegal immigrants who are uninsured. Based on this analysis it seems very likely that one of the primary effects of legalization would be to increase government-financed health care for former illegal immigrants. Thus, amnesty for illegal immigrants does not solve the problem of taxpayers providing health care to less-educated immigrants, even if it does increase insurance coverage among illegal immigrants.
Conclusion
This report estimates the size of the illegal population without health insurance and incomes low enough to qualify for the health insurance affordability credits contained in The America’s Affordable Health Choices Act of 2009 (HR 3200). Although the bill states illegal immigrants are not to benefit from the new affordability credits, this prohibition is without an enforcement mechanism. Congress voted down an amendment in committee that would have required the use of the SAVE program. Almost all other means-tested programs of the kind found in HR 3200 require the use of SAVE. As it now stands, the bill has a ban on illegal immigrants, but Congress has chosen to leave that ban unenforced. As a result, the nearly seven million uninsured illegal immigrants with qualifying incomes could receive affordability credits under the bill, creating billions of dollars in costs to taxpayers. If the final version of health care reform includes a public option plan and if illegal immigrants enroll in that program instead of receiving affordability credits, the costs would be less for taxpayers. Nonetheless, if the government became the direct insurer of illegal immigrants, the cost of covering them would still run into the billions of dollars.
End Notes
1 See page 4 of the CRS report “Treatment of Noncitizens in H.R. 3200,” at http://www.cis.org/sites/cis.org/files/articles/2009/CRS_Report_on_HR320....
2 See page 143 of HR 3200, at http://energycommerce.house.gov/Press_111/20090714/aahca.pdf.
3 See page 4 of “Treatment of Noncitizens in H.R. 3200,” at http://www.cis.org/sites/cis.org/files/articles/2009/CRS_Report_on_HR320....
4 The 207,000 persons in the Survey, 25,000 of whom are foreign-born, are weighted to reflect the actual size of the total U.S. population. However, it must be remembered that some percentage of the foreign-born (especially illegal immigrants) are missed by government surveys of this kind. The foreign-born are persons who are not U.S. citizens at birth. This includes naturalized U.S. citizens, legal permanent residents (green card holders), those on long-term temporary visas (e.g., foreign students and guest workers), and illegal immigrants.
5 To distinguish legal from illegal immigrants in the survey, we use citizenship status, year of arrival in the United States, age, country of birth, educational attainment, sex, receipt of welfare programs, receipt of Social Security, veteran status, and marital status to assign probabilities to each respondent. Those individuals who have a cumulative probability of one or higher are assumed to be illegal aliens. The probabilities are assigned so that both the total number of illegal aliens and the characteristics of the illegal population closely match other research in the field, particularly the estimates developed by the Department of Homeland Security/legacy INS, the Urban Institute, and Pew Hispanic Center. This method is based on well established facts about the characteristics of the illegal population. For example, it is well known that illegal aliens are disproportionately young, male, unmarried, have few years of schooling, etc. Thus, we assign probabilities to these and other factors in order to select the likely illegal population. In some cases, we assume that there is no probability that an individual is an illegal alien, such as a person who indicates that he or she is receiving Social Security payments or who is a U.S. veteran. The total number of illegals in the CPS is based on a residual analysis that uses administrative data to estimate the size and characteristics of the legal immigrant population and then subtracts those individuals from the foreign-born population in the survey.
6 The Department of Homeland Security (DHS) estimate of 11.6 million illegal immigrants in January 2008 can be found at http://www.dhs.gov/xlibrary/assets/statistics/publications/ois_ill_pe_20.... DHS’s estimate includes an adjustment for those missed by the Census Bureau. The Pew Hispanic Center has estimated a population of 11.9 million illegal immigrants as of March 2009 based on the CPS. Pew’s estimate also includes an adjustment for those missed by the survey. The Pew report can be found at http://pewhispanic.org/files/reports/107.pdf. The Urban Institute has calculated that, in March 2002, 8.3 million illegal aliens were in the United States, and one million were missed. Urban’s estimates based on the March 2002 CPS can be found at http://www.urban.org/url.cfm?ID=1000587. Older studies by the INS and Census Bureau are also available. An INS report found that there were seven million illegal aliens in 2000, with an annual increase of about 500,000 (www.immigration.gov/graphics/aboutus/statistics/Ill_Report_1211.pdf). The Census Bureau estimate of eight million illegals in 2000 can be found at www.census.gov/dmd/www/ReportRec2.htm (Appendix A of Report 1 contains the estimates).
7 See page 3, Table 2 in the DHS estimates of the illegal immigrant population for January 1, 2008, at http://www.dhs.gov/xlibrary/assets/statistics/publications/ois_ill_pe_20....
8 See Table 26 in Immigrants in the United States 2007, A Profile of America’s Foreign-Born Population, at http://www.cis.org/immigrants_profile_2007.
9 For a family of four in the continental United States, 133 percent of poverty equals about $29,000 a year and 400 percent of poverty equals about $88,000 a year.
10 See CBO letter to Charles Rangel (D-N.Y.), Chairman, House Ways and Means Committee dated July 17, 2009, at: http://www.cbo.gov/ftpdocs/104xx/doc10464/hr3200.pdf. See table on page 2.
11 In a letter to Rep. Rangel dated July 14, 2009, CBO shows how the affordability credit might work by income level. The largest subsides are for those with the lowest incomes. Table 2 in this report comes directly from the July 14 CBO letter. See page 2, at http://www.cbo.gov/ftpdocs/104xx/doc10430/House_Tri-Committee-Rangel.pdf.
12 In CBO’s July 14 letter to Rep. Rangel, they estimate that the net annual costs of the bill (savings minus new costs) would be $107 billion in 2014 and that this would grow to $171 billion by 2018.
13 Based on our analysis of the March 2008 CPS, we estimate that 78 percent of illegal immigrants with incomes under 400 percent of poverty and who are uninsured fall into the 18 to 40 age group. In contrast, 46 percent of legal immigrants and native-born Americans fall into this age group.
14 Although not the primary focus of this analysis, if the government directly insured illegal immigrants through a public option plan or Medicaid it could cost taxpayers roughly $10 billion a year. The Kaiser Family Foundation estimates that total expenditures from all sources for all uninsured people is $57.4 billion annually, this includes charity, self payments, and the $42.9 billion government payments. If illegals are receiving 10 percent of this total, then it comes to $5.74 billion. Kaiser also estimates that expenditures on lower- and middle-income uninsured would increase 70 percent if they had health insurance. Given the very low incomes of uninsured illegal immigrants, it is likely that the increase in their health care expenditures, once they are given insurance, would be higher than 70 percent. But assuming an increase of 70 percent, illegal immigrants could be expected to use roughly $10 billion in care annually. While this is a very crude estimate, it does indicate that direct coverage would be much less costly than providing indirect coverage in the form of affordability credits. Kaiser’s estimates can be found at http://www.kff.org/uninsured/upload/7810.pdf.
15 Kaiser’s estimate of governmental costs for treating the uninsured is for both part-year and full-year uninsured individuals in 2008. The CPS-based estimates used in this analysis are only for full-year uninsured. However, we assume that illegal immigrants represent the same fraction of part-year uninsured as they do full-year uninsured individuals. Most of the costs for treating the uninsured are for the year-round population. Kaiser’s estimate for the costs of the treating the uninsured can be found in “Covering the Uninsured in 2008: Key Facts about Current Costs, Sources of Payment, and Incremental Costs,” at http://www.kff.org/uninsured/upload/7810.pdf. Kaiser’s analysis also provides estimates for how much health care the uninsured would receive if they had insurance. Kaiser estimates that, if insured, health care expenditures for this population would rise 70 percent.
16 It is almost certain that illegal immigrants account for a larger share of the uninsured than 14.6 percent. Many native-born Americans and legal immigrants who respond to the CPS do not report their enrollment in Medicaid. Virtually no illegal immigrants should be on Medicaid. The 2008 CPS shows 39.6 million people on Medicaid. The Office of the Actuary at the Centers for Medicare & Medicaid Services reported 48.1 million people on Medicaid in 2007. See page 11 of the report, at www.cms.hhs.gov/ActuarialStudies/downloads/MedicaidReport2008.pdf. Some of the difference is accounted for by people on Medicaid in nursing homes, who are not counted by the CPS. Nevertheless, the overall size of the year-round uninsured population in the CPS should be several million smaller than the 45.66 million shown in the 2008 CPS. If we adjust for Medicaid undercount, then illegal immigrants would be 17 or 18 percent of the uninsured.
17 The March 2008 CPS shows 45.66 million uninsured people in the country, including immigrants (legal and illegal). The 6.67 million uninsured illegal immigrants represent 14.6 percent of that total. If we adjust the number of uninsured illegal immigrants upward by 10 percent, uninsured legal immigrants by 3 percent, and the uninsured native-born population by 1.5 percent, then illegal immigrants would total 15.6 percent of the uninsured. But with or without these adjustments, illegal immigrants are still about 15 percent of the uninsured in the United States. As already indicated, DHS uses a 10 percent undercount adjustment in estimates of the illegal population. For more detailed discussion of the undercount of the foreign-born in Census Bureau data by migration status see several reports by Jeffrey S. Passel, Jennifer Van Hook, and Frank D. Bean at http://sabresystems.com/sd_whitepapers_immigration.asp.
18 See “Births to Immigrants in America, 1970 to 2002,” at http://www.cis.org/ImmigrantsBirths-1970-2002.
19 This estimate is based on the younger age of illegals and the assumption that they create zero costs for programs that provide care to uninsured veterans and the Indian Health Services. The Department of Health and Human Services Medical Expenditure Panel Survey shows health expenditures by age group. We use this to estimate health care costs excluding those programs for the uninsured that illegals cannot use. If the undercount adjustment of Medicaid use in the CPS discussed in note 14 is made, immigrants would account for 11 or 12 percent of all costs for treating the uninsured.
20 Sherrie A. Kossoudji and Deborah A. Cobb-Clark, “Coming Out of the Shadows: Learning about Legal Status and Wages From the Legalized Population,” Journal of Labor Economics, vol. 20, no. 3, July 2002: 598-628.
21 Francisco L. Rivera-Batiz, “Undocumented Workers in the Labor Market: An Analysis of the Earnings of Legal and Illegal Immigrants in the U.S.,” Journal of Population Economics, February 1999.
22 Of this 81 percent, we estimate that 54 percent have not graduated from high school and another 27 percent have only a high school education.